Electrical hazards
Electrocution
The electricity main has one electrode connected to earth. This is cost-effective for power distribution, but creates a problem in that anyone touch the 'live' wire will receive an electric shock if they are in contact with any earthed point.
Traditionally, most electrical equipment was earthed. This provides protection in two ways: (Figure 1).
- The case is bonded to earth potential and so cannot be a source of shock
- Since there is a low resitance to earth, a very large current will flow (many times that used by the device when operating normally). This produces a heating effect. If a carefully chosen, thin piece of wire is placed on the 'live' side of the supply, then this will heat to melting point, breaking the circuit. For easy repair, these narrow wires are provided as components in their own right - i.e. fuses.
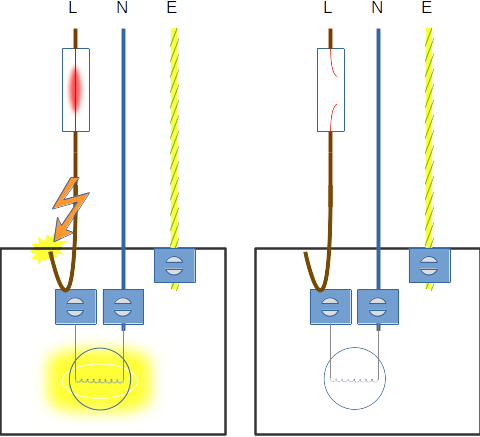
Live wire touches the equipment case. A large current flows to earth, causing the fuse to become hot, melt and break the circuit.
Modern equipment tends not to be earthed, making use of double insulation (any external metal parts are separated from any internal by a layer of insulation), but this this still leaves some possibility of electric shock.
The risk can be greatly reduced by isolating the mains supply from earth and this is possible using 1:1 wound transformers, where the output voltage is the same as the input (figure 3). This is an isolated power system (IPS).
Since the mains is earth referenced, touching the live wire will result in a shock (Fig. 3 - 1). The position for neutral is more ambiguous. Since neutral is connected to the earth at the sub-station, no shock should result. This depends on good connections all along the chain (i.e. low resitance to current flow) and also that no live/neutral wiring errors have occurred. It is not wise to try and test this (Fig. 3 - 2!!. The possibility of live/neutral wiring errors explains the latest requirement for fuses to be included in both the live and neutral lines and the resulting collection of fuses on the back of a modern anaesthtic machine.
On the secondary side of the transformer, there is a 240V potential difference between the output terminals, but since there is now NO earth connection(the coupling between the primary and secondary windings is magnetic, not electrical), there is no voltage between either terminal and earth (Fig. 3 - 3).
It is possible to touch either terminal (Fig. 3 - 4). What happens in this case is that the person (4) becomes the earch connection and defines the transformer terminal they are touching as earth. This is why the voltmeter on the other teminal will now read 240v to earth. Everyone else in theatre also reamins safe (5). Exactly the same is true if the postions are revered and a person (7) touches the other transformer terminal. This now becomes earthed. Touching BOTH terminals will still result in a shock - current will flow through the person in (8), quite indepedent of any earth connection.
An isolated power supply only adds an additional layer a safety. It cannot prevent shocks under all circumstance. If a fault exists (i.e. person 9 is in contact with a terminal), then when person 10 makes contact with the other termial, both will receive a shock the magnitude of which will depend on their relative resitances. This will happen because a complete circuit exists via the earth. To help prevent this, most IPS monitor the resitance to earth on each of the transformer terminals. As soon as the first fault occurs (e.g. Fig. 3 - 9) and alarm will sound. This should be an urgent cue to everyone in theatre to check the electrical devices (was something just plugged in / is there fluid dripping onto a power connector ?). The IPS is providing a warning that no further protection is available - the next fault may well result in shock !
In hospital, sockets connected to an IPS are often coloured differently and these should only be used with medical equipment. This is to minimise the load and the risk from faulty equipment.

An socket on an IPS system

An isolated power supply system
If the body is exposed to a potential difference, then the effects depend on how much current flows. This in turn depends on electrical resistance. Dry skin has a high resistance. Theatre clogs, although allowing leakage of static electricity, have a very high resistance and provide some protection against electric shock.
The presence of water or electrolyte solutions (e.g. iv fluids) results in a substantial reduction in resistance.
If currents can gain entry into the body (e.g. through invasive monitoring lines), then very small currents (micro-shocks) can produce VF.
| Current | Physiological effect |
|---|---|
| 150μA | Micro-shock - VF |
| 1mA | Threshold of feeling - tingling |
| 5mA | Maximum harmless current |
| 10-20mA | Tetany - can't release |
| 100-300mA | VF |
| 6A | Temporary respiratory paralysis Burns likely |
Classification of equipment
You will come across two classifications of electrical safety. The first describes the means by which electric shock is prevented and applies to all electrical equipment.
Class 1
Any metal part accessible to the user is earthed. If a fault develops such that a live wire touches the case, then the resulting current surge will blow a fuse, isolating the equipment. There is no standard symbol to identify Class 1 equipment.
Class 2
This is double-insulted equipment. Any metal accessible to the user is separated from live components by one layer of reinforced insulation or two non-reinforced layers. An earth wire is not required (but may be present for other reasons such as screening). Class 2 equipment can be identified by the symbol below.

Class 3
This is low-voltage equipment (<25V AC or 60V DC) which may be battery powered or powered by an external, isolating transformer. All medical equipment which is capable of being operated with a mains connection must be tested as Class I or Class II (Class III is not recognised). Equipment which operates on battery is referred to as 'internally powered'. You will find some operating tables which are capable of mains connection (for battery charging) but which should NOT be connected to the mains whilst in use; this is why.
The second classification is specific to medical equipment and describes the degree of protections which the design affords.
| Class | ||
|---|---|---|
| B | BF | CF |
 |
 |
 |
Type B
Equipment of type I,II or III where the applied parts are not isolated from the mains supply (i.e. not floating).
Type BF
Equipment of type I,II or III where all connections to the patient are via floating circuits. Not for direct cardiac connection.
Type CF
Equipment of type I,II or III where all connections to the patient are via floating circuits and which have a high degree of protection against leakage currents such that direct cardiac connection is safe.
With respect to electrical equipment:
- Double insulted equipment can be used in wet areas
- Class 1 equipment is double insulted
- The patient should be connected to earth
- Class 2 equipment is fully earthed
- Class 3 equipment is low voltage
Concerning electrical safety:
- Diathermy machines always require earthing
- Wetness decreases resistance
- Induced current is reduced by using saline to prime manometer tubing
- A current below 24mA is safe at the myocardium
- Risk of shock is increased with diathermy using floating patient circuits
Concerning electrical safety:
- The operating table should be earthed
- An intra-cardiac shock of $150 \mu A$ can cause systolic cardiac arrest
- Earthed mains equipment will always have a leakage current to earth
- Ventricular fibrillation can be caused by 50mA current
- Wet hands decrease resistance
FFTTT
The risk of AC electric shock is reduced by:
- A conducting floor
- Conducting shoes
- A humid atmosphere
- Using bipolar diathermy
- Electrically isolated patient
FFFFT
If an electric current is fed through the body:
- Risk of injury is largely dependent upon the current flow
- Antistatic shoes provide good protection due to their high resistance
- High frequencies are more dangerous than low frequencies
- Ventricular fibrillation occurs at a lower current in patients with dysrhythmias
- A tingling sensation is felt at a current strength of 1 mA
TTFTT
Concerning electrical safety:
- When touching faulty apparatus with wet hands, skin impedance is increased and current flow greater than normal
- Electrical shock is not a risk with potential below 24 V AC or 50 V DC
- The modern diathermy earthing plate is not connected directly with earth
- Micro-shock may lead to ventricular fibrillation via an intra-cardiac catheter with currents in excess of 150 micro amps
- Leakage currents are induced voltages in other circuits resulting from an alternating mains current
FTTTT